10 ANUSRI CASE STUDY -2
CASE STUDY
Oct 4 , 2021
This is an online e log book to discuss our patient identified health data shared after taking his/her guardian signed informed consent. Here we discuss our individual patient problems through a series of inputs from available global online community of experts with a aim to solve those patients clinical problem with collective current best evidence based inputs.
This blog also reflects my patient centered online learning portfolio and valuable inputs on the comments box is welcome.
I have been given this case to solve in an attempts to understand the topic of patient clinical data analysis, to develop my competency in reading and comprehending clinical data including history, clinical finding, investigation.
CASE:
69 year old female was brought to the causality with a complaint of sudden onset of aphasia preceded by 2 episodes of vomiting.She was apparently asymptomatic before.After then she had 2 episodes of vomiting and after which she had difficulty in speech, generalised weakness, staring look at times, difficulty in walking, walking with support, patient is unable to recognise her family members. She had similar episodes 10 days back i.e vomiting associated with weakness and disorientation. Patient was given adequate food and fluids at home and she became stable in 2 days.
Complaints and Duration:
sudden onset of aphasia preceded by 2 episodes of vomiting
Staring look
Associated with involuntary movements
rolling of eye balls
Tongue bite (-ve)
History of present illness:
Involuntary micturition and defecation
History of past illness:
Not a known case of diabetes Miletus, tuberculosis, hypertension, thyroid and asthmatics
No h/o seizures, head injury
No h/o substance abuse
No h/o fear, repetitive thought of action
Decrease in sleep, decrease in appetite
Self care and hygiene not maintained
Personal history:
Non alcoholic
Doesn’t smoke
Non vegetarian
Treatment history:
Not significant
General examination:
30/9/2021:
Conscious (confused)
Intermittent coherence
Speech: response to few commands
2/10/2021:
Irrelevant talk intermittently
No fresh complaints
4/10/2021:
Irritability and irrelevant talk reduced
Patient is able to recognise family members at times and hallucinating behaviour decreased
Vitals:
30/10/2021:
BP: 120/60 mm Hg
PR: 84bpm
1/10/2021:
Temp: Afebrile
BP:110/60mm Hg
PR: 88 bpm
2/10/2021:
Temp: 97.5 F
BP: 120/60mm Hg
PR: 86 bpm (regular)
3/10/2021:
Temp 97.5 F
BP: 110/80mm Hg
PR : 88bpm regular
Systemic examination:
1/10/2021:
CVS: S1 S2 + no murmur
RESP SYS: Resonated breath sounds in B/L ISA
P/A - soft, no tenderness
CNS:
RT LT
TONE: UL: 2/5 2/5
LL: 2/5 2/5
POWER: UL: 2/5 2/5
LL : 2/5 2/5
REFLEX: B T S A K P
- - - - - F
- - - - - F
2/10/2021:
CVS: S1S2 + Nomurmur
Rs: NVB1 decreased breath sounds in lt RSA
P/A soft, no tenderness
I/O 2200/1600 ml
GRBS 152 mg/dl
3/10/2021:
CVS: S1S2 + Nomurmur
Rs: NVB1 decreased breath sounds in lt RSA
P/A soft, no tenderness
I/O 1550/1400 ml
GRBS 150mg/dl
Medication chart:
1/10/2021:
INJ.PAN 40mg i.v OD
INJ.ZOFER 16mg i.v SOS
TAB. DOLO 650mg PO OD
INJ.OPTINEURO 650mg OD
INJ.MONOCEF 1g I.v OD
2/10/2021:
INJ. PAN 40mg I.v OD
INJ.ZOFER 4mg I.v SOS
TAB. DOLO 650mg PO SOS
SYP.ABROXY 10 mg PO TID
INJ.MONOCEF 1g I.v BD
TAB.ADMENTA 10mg PO OD
TAB.OLANZAPINE 5mg PO OD
3/10/2021:
INJ.PAN 40mg I.v OD
INJ.ZOFER 4mg I.v SOS
INJ.MONOCEF 1g I.v BD
INJ.DOLO 650mg PO SOS
SYP.AMBROXYL 10ml PO SOS
TAB.OLANZAPINE 5mg PO OD
4/10/2021:
INJ.PANTOP 40mg i.v OD
INJ.ZOFER 4mg i.v SOS
TAB.DOLO 650mg PO TID
SYP.AMBROXYL 10ml PO TID
INJ.MONOCEF 1g I.v BD
TAB.ADMENTA 10mg PO OD
TAB.OLANZAPINE 2.5mg PO OD
INJ.HALOPERIDOL 1/2amp/I.M/SOS(if patient is irritable)
INJ.LACTULOSE 15ml/PO/HS
IVF (NS and RL) 75ml/hr
1amp of OPTINEURON I.v OD
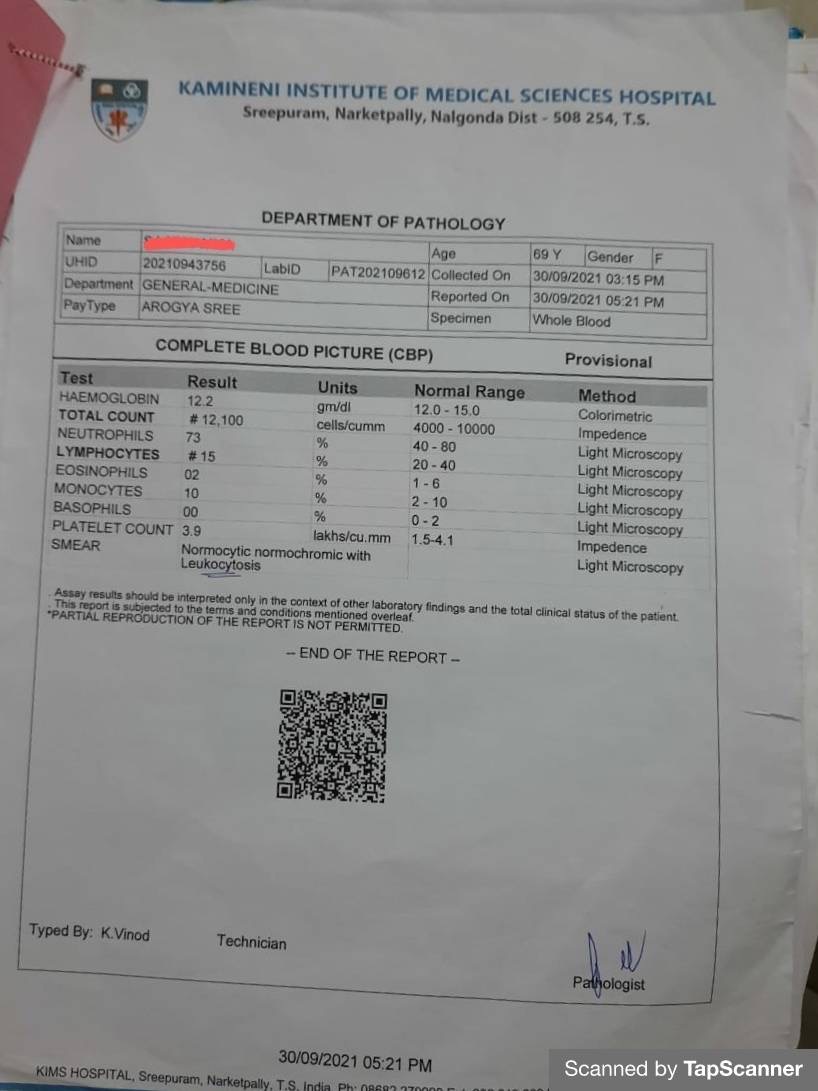
INVESTIGATIONS:
1. COMPLETE BLOOD PICTURE:

3. CBP, serum electrolytes, LFT

4. ECG

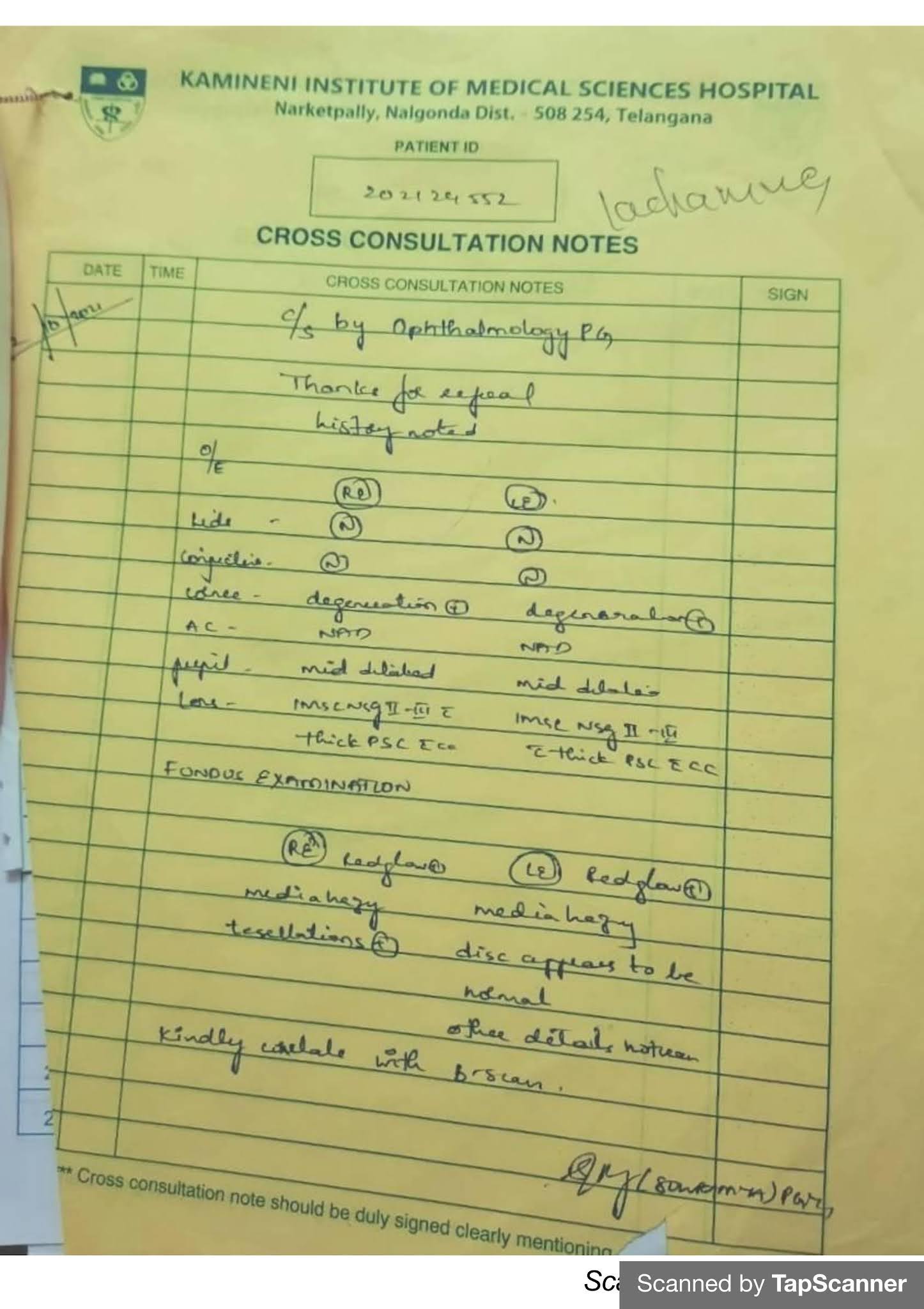
OTHER INVESTIGATIONS:

PROVISIONAL DIAGNOSIS:
Wernickes Aphasia


Comments
Post a Comment